Acoustic Reflex Testing
Tympanometry Guides
What is the acoustic reflex?
The acoustic reflex consists of a response by one or more middle ear muscles to suprathreshold acoustic stimulation of the auditory pathway. To elicit an acoustic reflex, an acoustic stimulus (pure-tone, noise, or click) is presented to the ear canal by a probe or earphone. A portion of this stimulus is carried by the ossicular chain to the cochlea. From the cochlea, the 8th nerve carries the information to the brain stem where a determination is made as to whether the stimulus is sufficiently intense to elicit a response. When a response is elicited, the 7th nerve carries the command to the stapedius muscle to contract. Contraction of this muscle and/or the tensor tympani stiffens the eardrum and the ossicular chain; thereby, decreasing the ease with which sound enters the auditory pathway. Thus, the end result of an acoustic reflex is a slight decrease in the ability of the eardrum and the ossicular chain to conduct acoustic energy to the cochlea.
Acoustic Reflex Test
Since the acoustic reflex causes a relatively small decrease in mobility (0.02 ml or greater using a probe tone of 226 Hz) within the middle ear system, it is important to conduct this test at a pressure level where the greatest response occurs. Therefore, acoustic reflex threshold and decay measurements are generally carried out at the pressure value where peak mobility occurred during a tympanogram. If no peak is observed, the acoustic reflex tests are performed at atmospheric pressure (0 daPa).
Acoustic reflex measurements can be obtained Ipsilaterally or Contralaterally. For Ipsilateral testing, the stimulus is presented to the same ear where the measurements are made. For Contralateral testing, the measurements are made with the probe in one ear while the stimulus is presented to the opposite ear through an earphone or insert phone.
Reflex Decay Testing
Reflex Decay is a diagnostic test particularly useful in confirmation of retrocochlear pathology. The stimulus for the test is typically presented as a steady tone contralaterally at 10 dB HL above reflex threshold intensity level. The test frequencies of choice are 500 and 1000 Hz.
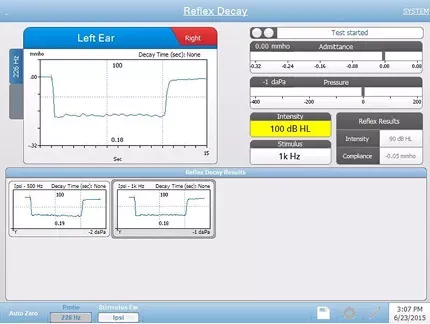
An individual exhibits adaptation (decay) if the amplitude of the reflex response decays to 50% of peak amplitude typically within 10 seconds.
Acoustic Reflex Latency Test (ARLT)
In broad terms, Acoustic Reflex Latency is the time interval between the onset of an acoustic stimulus and the onset of the stapedius muscle contraction. Investigators have reported prolongation of latency with retrocochlear disorders. There is an awareness that the Acoustic Reflex Latency Test (ARLT), a simple clinical procedure, can be a sensitive indicator in distinguishing cochlear from retrocochlear lesions. Interest has focused on latency characteristics, rise and fall times of the reflex response, amplitude, and recovery characteristics. The definitions of these parameters are variable among investigators.
Acoustic Reflex Latency is dependent on frequency, intensity, and rise/fall times of the eliciting stimulus. The protocol for this test requires the presentation of an Ipsilateral or Contralateral reflex-activating stimulus (rise time equal to or greater than 5 msec.) at 10 dB above acoustic reflex threshold level. Averaging the reflex responses improves the signal/noise ratio and thus smoothes the displayed response.
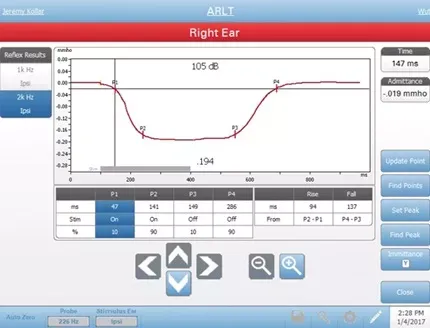
TympStar – this method uses the calculations that were used by the GSI TympStar. Four data points are marked that correspond to the 10% and 90% of the maximum amplitude from the stimulus onset and the 10% and 90% response decay from the stimulus offset. The rise and fall times are calculated from the marked points.
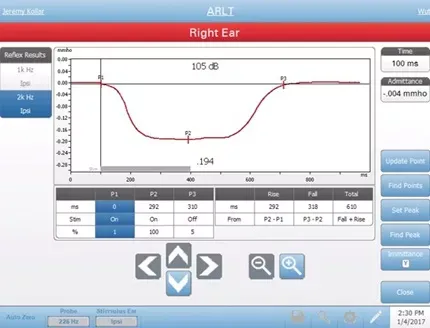
Norris – this method uses a different calculation based on the reference below and marks 3 data points. The 3 points correspond to the initial deflection after the start of the stimulus, the maximum amplitude and the 95% response decay from the stimulus offset. The rise, fall and total times are calculated from the marked points.
Norris, et. al, “Latency Measures of the Acoustic Reflex”, Audiology 13: 464-469 (1974)