An Introduction to the ACT Test

The newly available ACT™ (Audible Contrast Threshold) test is a fast, language-independent, proxy for aided speech-in-noise testing. The results are useful for patient counseling, hearing aid selection, and setting the advanced signal processing features of hearing aids. Let’s look at how the test works and go over some tips on how to implement the ACT test into your practice and avoid some common pitfalls.
In a nutshell, the ACT test is a clinical test measuring binaural spectro-temporal modulation sensitivity to quickly quantify a person’s real-world ability to understand speech-in-noise. The patient’s task is to discriminate between the modulated noise and non-modulated noise. During testing, the non-modulated noise is playing continuously in the background while we introduce varying levels of modulated noise to find the Contrast Threshold, or lowest amount of modulation that can be detected by the patient. The resulting Contrast Threshold has a good correlation with aided speech-in-noise performance, and acts as a language independent proxy (substitute) for an aided speech-in-noise test.
To perform ACT testing, the first thing you need is a calibrated audiometer with air conduction transducers (inserts, phones and/or HF phones) that has been licensed for ACT testing. GSI has two audiometers that can perform the ACT test; AudioStar Pro™ and the Pello™. The test comes standard with new AudioStar Pro devices, and an additional license (Speech Plus) is required for use with new Pello devices. *Reach out to your local specialty equipment distributor if you have questions about ACT licensing and availability.
Next, ACT testing requires the use of a patient response button. The task for the patient is to press the button when they hear the modulated noise (siren like sound) during testing. Those response, non-responses, and false positives are then automatically plotted on-screen during testing, so a response button is essential.
A key component to getting a valid ACT test result is the audibility of the modulated noise during testing. To ensure the stimulus is audible to each patient, we need to have an audiogram saved on the audiometer prior to testing. These thresholds are used to determine the frequency response and intensity of the ACT testing stimulus (modulated noise) individually for each patient. Air conduction pure tone thresholds must be obtained bilaterally at the required frequencies of 250, 500, 1000, 2000, and 4000 Hz. Other frequencies can be included in testing, but to proceed with the ACT test we need these octaves stored at minimum.
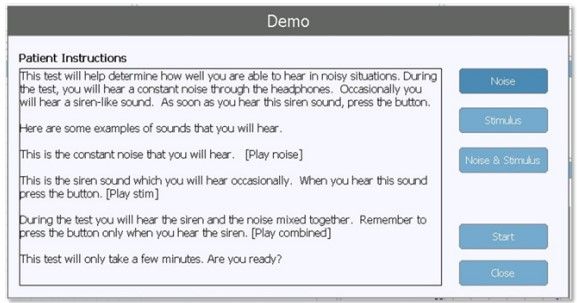
Once we have met our prerequisites, ACT testing can begin. The ACT test is located in the “More” test type. When we navigate to the ACT special test on the audiometer, a “Patient Instructions” dialog will appear that allows us to play examples of the non-modulate noise, modulated noise (target stimulus), and the two mixed together prior to testing to familiarize them with the task.
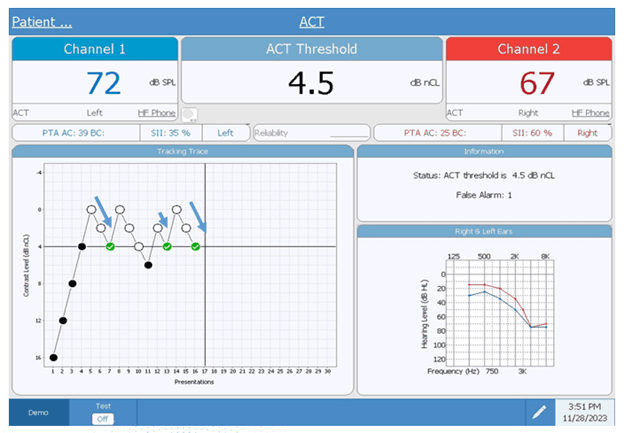
Once the dialog is dismissed, testing automatically begins and the non-modulated noise begins playing on both ears. To administer the test, the examiner will press the presentation button to present the modulated noise stimulus to the patient. Beginning at a Contrast Level of 16 dB nCL (normalized contrast level), we use a bracketing technique to determine a threshold. For each response, we go down 4 dB nCL in intensity. For each non-response, we go up 2 dB nCL. The ACT threshold is obtained when 3 responses at a single contrast level are recorded on ascending intensity presentations of 2 dB. The responses must be within 5 turning points or responses. This method is key, and we will expand on it a little later. When this criterion is met, the test automatically stops, and the ACT threshold will be displayed on screen.
In this example the ACT threshold is 4.5 dB nCL.

 response
response
 no response
no response
 threshold
threshold
The test in this example took about 2 minutes to complete, and that is close to the overall average test time for the ACT test. However, just as with any threshold test, some people will struggle with consistency when the stimulus is close to their threshold, and it can become quite difficult. That, along with other factors such as confusion about the task, can lead to what we call “extended runs” where we are over 25 presentations in and a threshold has not been determined. When testing exceeds 25 runs, an automatic warning pops-up on screen to encourage a break in testing. Once a run extends beyond 25, the reliability of test can decrease, and the patient can become exhausted by the testing.
To avoid lengthy test times, there are a couple of things to focus on for success. Beginning with the instructions, make sure your patient clearly understands what to do. Emphasize that the background noise will be playing in both ears during the entire test, that it is important to concentrate throughout to listen for the “siren-like” noise, and to press the button as soon as they hear it. Play the samples multiple times, if necessary, before beginning.
Another key is making sure to follow the bracketing procedure exactly. One of the rules for establishing threshold is that responses are within “5 turning points” on ascending intensity. In this next example, we can see some common mistakes made in presenting the stimulus, including the following:
![]()
In the example above, the ACT testing starts off good. The bracketing rule is being followed through the first 8 presentations but instead of descending 4 steps (in this case only 2 steps as the limit is -2), another presentation is made at the same intensity, and then another. This effectively eliminates the threshold candidate from consideration at -2 that was established in presentation number 6, adding to the time necessary to establish a threshold.
To avoid longer test time, make sure to always ascend in 2 dB steps following the no-response to quickly come to a threshold:
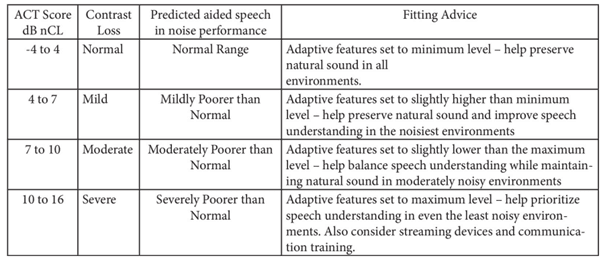
There are several benefits to using the ACT. First and foremost, the ACT threshold can be used to help select and then program the advanced features of hearing aids, improving patient outcomes. Hearing aids made by Oticon, Bernafon, Sonic, and Phillips can directly import the ACT threshold in their fitting platforms, and the software will automatically optimize the adaptive features of hearing aid such as noise reduction and directionality. Additional fitting advice has been produced for brands other than the above mentioned to use the ACT threshold to help guide programming of these advanced settings:
Second, the ACT test is language independent. For some, this might be the biggest benefit. If your clinic serves a diverse population of adults, it can be a challenge to deliver a full audiologic battery of tests, especially when it comes to speech-in-noise testing. The ACT gives us a predicted aided speech-in-noise performance information, and having this as tool for testing with non-native English speakers is a game-changer.
The last big benefit is time. The average test time is just a couple of minutes to determine threshold. This is important because the ACT test is not meant to replace traditional speech-in-noise testing or any other part of the diagnostic battery. It is a new tool that should be considered another piece of diagnostic puzzle giving us a more complete picture to move forward with. I realize that many of us are already strapped for time for testing, but building in a few extra minutes to obtain valuable information that can help set realistic expectations and improve fitting outcomes makes incorporating ACT into your protocol worth it.
Additional information about the ACT test can be read on the Oticon website.
Interested in GSI resources? Download the ACT FAQ and Quick Guide here: Audible Contrast Threshold Test | Grason-Stadler
Tony received his master’s from the University of Wisconsin-Oshkosh with an emphasis on pediatric audiology. He has over 20 years of experience in the hearing industry and has worked in a variety of settings. He has experience performing diagnostic testing with all age ranges, industrial audiology, retail, hearing aid financing and insurance, practice development programs and industry trade shows. At GSI, Tony is focused on training, support and education.


